
Chronic Pain
Chronic Pain
Last Section Update: 04/2024
Contributor(s): Shayna Sandhaus, PhD
1 Overview
Summary and Quick Facts for Chronic Pain
- Chronic pain can drastically reduce quality of life and is often resistant to medical therapies. Opioid medications are addictive and have the potential to ruin lives, if not used very judiciously. Excessive use of NSAIDs like ibuprofen increases risk of many health problems.
- In this protocol, learn about the risks of long-term pharmaceutical pain management strategies. Also discover that several natural compounds have been shown to target some of the fundamental mechanisms of pain, to provide relief without debilitating side effects.
- A supplement called palmitoylethanolamide (PEA) has been shown in several clinical trials to reduce pain due to a variety of causes. PEA modulates inflammatory signaling and interacts with the body’s endocannabinoid system but does not cause psychotropic effects.
What is Chronic Pain?
Chronic pain, unlike acute pain, can last for months or even years. Chronic pain can drastically reduce quality of life, and unfortunately it is not always easy to determine the factors contributing to the pain.
Conventional medical treatments are wrought with adverse side effects, such as opioid addiction. Even over-the-counter drugs have been linked to adverse effects—acetaminophen overdose is the leading cause of acute liver failure in the United States.
Pain can be broadly classified as nociceptive (resulting from activation of peripheral pain receptors) or neuropathic (resulting from injury or dysfunction in the nervous system). Nociceptive pain is intrinsically linked with inflammation, while neuropathic pain may be more difficult to treat.
Natural interventions such as honokiol and palmitoylethanolamide (PEA) may help relieve pain without the adverse effects common to pharmacologic pain therapy.
What are Conventional Medical Treatments for Chronic Pain?
Non-pharmacologic:
- Exercise
- Behavioral therapy
- Meditation
- Biofeedback, and others
Pharmacologic:
- Non-opioid pain relievers (eg, acetaminophen and/or non-steroidal anti-inflammatory drugs [NSAIDs])
- Opioids
- Antidepressants (eg, tricyclics and serotonin-norepinephrine reuptake inhibitors [SNRIs])
- Antiepileptic drugs (eg, gabapentin, pregabalin, and other anticonvulsants)
- Muscle relaxants (eg, benzodiazepines)
- Topical analgesic agents
What Dietary Changes Can Be Beneficial for Chronic Pain?
Several types of dietary interventions have been linked with pain relief:
- Periods of fasting
- Low glycemic index diet (ie, high protein, low carbohydrate)
- Vegetarian/vegan diets
- Diet rich in antioxidants (fruits and vegetables)
What Natural Interventions May Be Beneficial for Chronic Pain?
- Honokiol. Honokiol, a polyphenol extracted from the bark of magnolia trees, has long been used to improve sleep and relieve anxiety. It may also help relieve inflammatory pain.
- Palmitoylethanolamide (PEA). PEA, a lipid present in tissues around the body, may be effective for relieving pain from many causes without adverse effects. Many clinical trials have demonstrated its effectiveness.
- Omega-3 fatty acids. Greater dietary intake of omega-3 polyunsaturated fatty acids has been linked to a reduction in both inflammatory and neuropathic pain.
- Gamma linolenic acid (GLA). GLA, a plant-derived omega-6 fatty acid that helps modulate inflammation throughout the body, has been shown to relieve pain from a variety of conditions.
- B vitamins. Vitamins B1 (thiamine), B6 (pyridoxine), and B12 are beneficial for many painful diseases. A mixture of these vitamins has also been shown to reduce neuropathic pain.
- Vitamin C. Evidence suggests free radicals play a role in exaggerated pain hypersensitivity. Several animal and clinical studies indicate vitamin C may help relieve nociceptive pain.
- Vitamin D. Vitamin D metabolites help inhibit inflammation. Deficiency is linked with several painful conditions. Administration of vitamin D was found to reduce pain for women with chronically painful periods and may help relieve pain from other causes as well.
- Curcumin. Curcumin has been shown to have analgesic effects and may be useful for a variety of pathological pain conditions. It reduces levels of inflammatory mediators involved in nociceptive pain hypersensitivity.
- Ginger. Ginger has analgesic and anti-inflammatory properties. Certain species can be helpful in reducing pain from muscle sprains, arthritis, menstruation, and others.
- Melatonin. Aside from its well-known role as “the sleep hormone,” melatonin is also a potent antioxidant and has been shown to reduce the pain associated with a variety of chronically painful conditions (eg, fibromyalgia, irritable bowel syndrome, and migraine).
- Additional natural compounds that may be helpful for managing chronic pain include vitamin E, proanthocyanidins (such as from grape seed), methylsulfonylmethane (MSM), and others.
2 Introduction
The sensation of pain arises in the nervous system. It has a variety of causes, but the experience of pain is variable and subjective.
Pain is both acute as well as chronic.
Acute pain is a protective mechanism that makes you aware of an injury (NIH MedlinePlus 2012; Cleveland Clinic 2008).
In contrast to acute pain, chronic pain is persistent and can last for months or years. Chronic pain can drastically reduce quality of life. We now know that 79% of chronic pain patients report disruptions in daily activities and 67% indicate that chronic pain negatively impacts their personal relationships (NIH MedlinePlus 2012; MedicineNet 2012; Vo 2008).
Chronic pain is often resistant to conventional medical treatments (MedicineNet 2012; Lumley 2011; Coluzzi 2011). Moreover, pharmacologic pain management of chronic pain is hindered by grave long-term side effects.
Opioids are wrought with adverse effects and have significant addiction potential, but poorly appreciated is that even over-the-counter pain medicines like acetaminophen and ibuprofen are linked with liver damage, kidney damage, and even heart attack (Woodcock 2009; Peterson 2010).
In this protocol, you will learn about the risks of long-term pharmaceutical pain management strategies. You will also discover that several natural compounds have been shown to target some of the fundamental mechanisms of pain to provide relief without debilitating side effects.
3 Understanding Pain
Acute pain follows a predictable, finite pattern and is generally short-lived, self-limiting, as well as easy to diagnose and treat. Pain that persists for longer than three months, and is not progressively better, is referred to as "chronic". It can be difficult to pinpoint the exact factors that cause chronic pain to persist over time (Lumley 2011).
Although there are many ways to organize different types of pain, one of the most popular and accepted schemes utilizes the following eight classifications to differentiate pain complaints (Smith 2005):
| Classification of Pain | Examples |
|---|---|
| Severity | Mild, Moderate, or Severe |
| Duration | Acute or Chronic |
| Location | Lower back, Abdomen, or Head |
| Origin | Nociceptive or Neuropathic |
| Body system | Muscular, Neurologic, or Skeletal |
| Mechanism | Central or Peripheral |
| Diagnosis | Cancer or Non-cancer |
| Response to treatment | Opioid-responsive or Opioid-resistant |
There are 2 major categories of pain; nociceptive and neuropathic (NINDS 2012):
Nociceptive pain guards the body against potential injury. It occurs as a result of the activation of peripheral pain receptors called nociceptors, which are activated by injurious stimuli. The stimuli is converted into an electrical signal, which is conveyed along nerve cells into the spinal cord or brain, where it is perceived as an unpleasant sensation (Cohen 2011).
Neuropathic pain occurs as a consequence of either injury or dysfunction in the nervous system. It produces a variety of unusual pain sensations that have been described as burning, crushing and "pins & needles." Unlike nociceptive pain, neuropathic pain often persists for prolonged periods of time, even after the original trauma and/or dysfunction is addressed (Costigan 2009). Since neuropathic pain is more complex than nociceptive pain, it is consequently more difficult to treat (Vorobeychik 2011).
4 Nociceptive Pain and Inflammation
Inflammation and nociceptive pain go hand-in-hand.
Inflammation is initiated upon tissue injury and sets off a cascade of biochemical reactions that prime the nervous system for pain sensing. Moreover, long-term inflammation reinforces adaptive changes in the nervous system that can cause the sensation of pain to become exaggerated or inappropriate (Ji 2011). For example, inflamed tissue (e.g., an arthritic knee) may be excessively tender and even a light touch might cause pain, a phenomenon known as allodynia.
Nociceptive pain does not occur spontaneously, it must be triggered within the nervous system. This task is accomplished by specialized receptors called nociceptors.
When you experience an injury, several inflammatory mediators including prostaglandins, tumor necrosis factor-alpha (TNF-α), interleukin 1β (IL-1β), and interleukin-6 (IL-6) are released at the site of the injury and interact with nociceptors, facilitating the transmission of pain signals through the nervous system. If you have a chronic inflammatory condition (e.g., osteoarthritis), then increased levels of inflammatory mediators at the affected site (e.g., a joint), as well as systemically, predispose you to increased pain sensations.
Therefore, taking steps to ease inflammation is an effective means of interfering with the process of pain sensitization. This is why drugs like acetaminophen (the active ingredient in Tylenol®) and ibuprofen, which are anti-inflammatory in nature, relieve pain. Unfortunately, though these drugs and others like them are very effective for reducing inflammation and pain, they often cause alarming side effects, which compromises their long-term risk vs. benefit profile (see The Potentially Lethal Side Effects of Over-the-Counter Pain Medications; below).
A variety of natural anti-inflammatory compounds are able to target inflammation by reducing the synthesis of inflammatory mediators, or modulating inflammatory pathways. As will be discussed later, many natural compounds exert powerful anti-inflammatory activity without causing unwanted side effects. See section titled "Targeted Nutritional Interventions".
5 Pain Management
The scientific approach to pain management demands a step-wise approach, which utilizes lower risk interventions first. In many cases, these lower-risk interventions are helpful for relieving chronic pain. For example, a recent review found that exercise and behavioral therapy were effective at decreasing pain and increasing functioning among patients with chronic pain (Hassett 2011). Other nonpharmacologic interventions that may be useful for chronic pain include meditation, biofeedback, acupuncture, electrical stimulation, and surgery (NIH MedlinePlus 2012). However, in those cases that do not respond to initial pain management treatment options with lower risk interventions, patients with chronic pain may have no other choice but to initiate pharmacologic therapy.
Pharmacologic therapy is one of the most popular treatment options for managing chronic pain. While initial treatment recommendations will vary based upon diagnosis (e.g., nociceptive vs. neuropathic), the most commonly used agents include (Bajwa 2012):
- Non-opioid analgesics (acetaminophen and/or NSAIDs)
- Opioids
- Antidepressants (tricyclics and serotonin-norepinephrine reuptake inhibitors [SNRIs])
- Antiepileptic drugs (gabapentin, pregabalin, and other anticonvulsants)
- Muscle relaxants
- Topical analgesic agents
Despite the wide variety of pharmacologic therapies available for patients with chronic pain, a recent report published by an international panel of experts has pointed out that current conventional treatment schemes are lacking in efficacy and often impose unacceptable side effects (Coluzzi 2011). For example, opioids are the most commonly prescribed class of medication in the United States for short-term relief of chronic pain, and yet, their efficacy and negative side effect profile have many experts questioning their use in this way; especially since the increase in opioid availability has been accompanied by an epidemic of opioid abuse and overdose (Von Korff 2011; Friedrich 2012). In addition to the potential for dependence, patients beginning opioid therapy should also be aware of other common side effects, which include (Friedrich 2012):
- Constipation
- Nausea
- Excessive sleepiness
- Itchiness (i.e., pruritus)
- Headache
- Respiratory depression
According to the World Health Organization’s (WHO) "analgesic ladder", opioids are not recommended for chronic pain unless the pain can be described as moderate to severe, and/or has not responded to previous (non-opioid) treatment approaches. Consensus xxpert guidelines only recommend opioid therapy for managing chronic (non-cancer) pain once all other reasonable lower risk and lower cost pain management interventions have failed (WHO 1990; Chou 2009).
In an effort to reduce the risk of serious adverse outcomes associated with narcotic pain relievers, Congress has recently mandated that the FDA create the Risk Evaluation and Mitigation Strategies (REMS), which requires drug companies to develop special educational programs for physicians and for patients who are prescribed these potentially dangerous medications (Okie 2010). While opioid therapy can be used for chronic (non-cancer) pain in a safe way, it must be initiated properly, and only in select patient populations (i.e., physicians should carefully screen for mental disorders and history of substance abuse) (Edlund 2007; Chou 2009).
Centrally-acting Drugs for Pain Relief
Chronic activation of peripheral pain sensors (nociceptors), such as occurs in osteoarthritis, for example, can alter central neural pain processing over time. The ongoing nature of chronic pain, and the adaptive nature of the central nervous system both contribute to biochemical alterations that increase pain sensitivity and cause the brain to become accustomed to processing pain. This phenomenon is known as central sensitization.
When the central nervous system has become "sensitized" to pain, painful sensations can be augmented because they are no longer only a nociceptive response, but are now being reinforced by mechanisms within the brain and spinal cord (Mease 2011).
Thus, chronic pain has a peripheral and a central element.
Evidence shows that patients with osteoarthritis of the knee are more sensitive to pain at other sites on their body than are healthy controls (Bradley 2004). This is because the brains of people afflicted with chronic pain have adapted to processing pain and have become hyper-responsive to painful stimuli.
The central element of chronic pain does not respond to traditional therapies such as anti-inflammatory drugs because they cannot modulate the transmission of pain within the sensitized central nervous system. Therefore, drugs such as antidepressants and antiepileptics can complement traditional anti-inflammatory drugs by modulating central biochemistry.
In the case of antidepressant drugs, it appears that the mechanism by which they provide pain relief is somewhat independent from their mood-altering affects (McCleane 2008), while antiepileptics alter pain signaling by modulating calcium signaling in the brain, which is also a mechanism by which they control seizures (Mease 2011).
For many people with chronic pain, centrally acting drugs are effective adjuvants to traditional pain therapies. Moreover, because central processing is a critical element of neuropathic pain, centrally-acting drugs are a mainstay of treatment in this setting (Yalcin 2009).
6 Nutrition and Pain
Diet
Recent evidence suggests that certain types of dietary interventions may have significant effects on chronic pain, especially severe forms of chronic pain (Tennant 2011). Also, chronic pain can result in a decreased protein intake and increased sugar and starch intake. These dietary changes result in wasting (i.e., catabolic state) (Tennant 2011).
Although the exact parameters of an "anti-pain" diet have not yet been recommended by any clinical organization (Tennant 2011), the scientific literature contains plenty of data indicating a strong link between food and pain. For example, periods of dietary fasting has been linked to the temporary relief of pain among many patients (Bell 2007). For longer term pain relief, some experts suggest a high protein, low carbohydrate diet (i.e., low glycemic index), which has been associated with decreases in pain sensitivity and inflammation (Ruskin 2009). Likewise, several studies have shown that a vegetarian/vegan diet is also beneficial to patients with chronically painful conditions (Bonakdar 2009).
Consuming a diet rich in antioxidants may also be helpful for the relief of chronic pain. This is because antioxidants neutralize free radicals and oxidative stress, which play a significant role in persistent pain conditions and have been linked to an increase in pain sensitivity (Tall 2004).
Some researchers believe that many of these dietary interventions activate the endogenous opioid system, which is the body’s natural defense against pain (Bell 2007). Moreover, documenting dietary history to ensure adequate protein intake can help chronic pain patients avoid muscle loss and weakness (Tennant 2011).
7 Nutrients
Honokiol
Honokiol is a polyphenolic compound from the bark of the magnolia tree (Magnolia grandifolia). Magnolia bark extracts have been used traditionally as sedatives to improve sleep and relieve anxiety, and honokiol is being investigated for its potential usefulness in treating inflammatory pain (Alexeev 2012; Woodbury 2013).
Like other polyphenols, honokiol has oxidative stress-reducing and anti-inflammatory activities. In addition, it appears to cross the blood-brain barrier and interact with certain neurotransmitter receptors in the brain (Woodbury 2013; Alexeev 2012). Laboratory research shows honokiol and some of its derivatives activate certain GABA receptors (Bernaskova 2015), and may also interact with receptors for glutamate, dopamine, and serotonin, and influence acetylcholine signaling (Alexeev 2012). One form of honokiol has even been shown to stimulate cannabinoid receptors that may be involved in decreasing pain perception (Gertsch 2012).
In one study, treatment with honokiol reduced pain-related behaviors in mice in experimental models of inflammation (Lin 2009). Findings from other animal studies indicate honokiol may decrease acute inflammatory pain without causing motor or cognitive side effects, and may prevent and decrease some of the chronic pain-related changes in the brain (Woodbury 2015; Lin 2007).
Palmitoylethanolamide
Palmitoylethanolamide (PEA) is a lipid compound that occurs naturally in tissues throughout the body, including the central nervous system. It can also be found in foods such as soy lecithin, egg yolk, and peanuts (Mattace Raso 2014; LoVerme 2005). A growing body of research suggests PEA supplementation may be effective for relieving pain from a variety of causes without triggering adverse side effects (Artukoglu 2017; Paladini 2016; Gabrielsson 2016). Most of the existing preclinical research indicates that PEA works by changing the expression of certain genes and reducing inflammatory signaling, but other possible mechanisms for its analgesic effect have also been proposed, including its ability to stimulate signaling through cannabinoid receptors in the nervous system (Gabrielsson 2016; Di Cesare Mannelli 2013; Skaper 2012; Khasabova 2012).
Several clinical trials have shown that PEA can reduce pain from a broad array of causes, including diabetic neuropathy, chemotherapy-induced peripheral neuropathy, sciatic nerve compression, carpal tunnel syndrome, osteoarthritis, low back pain, failed back surgery, stroke-related nerve pain, multiple sclerosis, dental pain, chronic pelvic pain, post-herpetic neuralgia, and vaginal pain (Hesselink 2012). In an observational study of individuals with chronic pain due to a variety of conditions who were unable to control their pain with usual therapies, adding 600 mg PEA twice daily for three weeks followed by once daily for another four weeks decreased average pain intensity scores in all participants who completed the study (Gatti 2012).
In a randomized controlled trial, 636 participants with pain due to compression of the sciatic nerve received either 300 mg PEA daily, 600 mg PEA daily, or placebo in conjunction with their usual pain medications for three weeks. Both doses of PEA resulted in greater pain reduction than placebo, and the higher dose was more effective than the lower dose. In fact, those in the 600 mg group experienced more than a 50% reduction in pain scores (Keppel Hesselink 2015). In 118 patients with nerve pain, 30 days of standard treatment plus 600 mg PEA daily was more effective than standard treatment alone (Dominguez 2012). A randomized clinical trial found that 900 mg PEA daily for one week followed by 600 mg daily for one week was more effective than ibuprofen, at a dose of 600 mg three times daily for two weeks, for relieving temporomandibular joint (TMJ) pain (Marini 2012).
Micronized preparations of PEA have also been studied. Micronization results in smaller particles that may be absorbed more readily. Micronized PEA, at doses of 600–1,200 mg/day, reduced pain in subjects with diabetes- or trauma-related nerve pain, chronic pain after failed back surgery, and acute pain from tooth extraction (Cocito 2014; Paladini 2017; Bacci 2011). In a report of 100 cases of nerve pain related to spinal disorders, the inclusion of an ultra-micronized PEA supplement in pain management therapy showed promising results (Chirchiglia 2017). A meta-analysis found that women with chronic pelvic pain due to endometriosis appear to benefit from the combination of 800 mg micronized PEA daily plus 80 mg per day of polydatin, a natural free radical-reducing agent found in grapes and red wine (NIH 2017; Indraccolo 2017). In a randomized controlled trial, the combination of PEA and polydatin was more effective than placebo for reducing abdominal pain in irritable bowel syndrome patients (Cremon 2017).
Omega-3 Fatty Acids
Fatty acids are essential nutrients derived from dietary intake of fats. They are an important source of energy for the body, and serve a variety of other biologic functions.
Greater dietary intake of omega-3 polyunsaturated fatty acids (PUFAs) has been linked to a reduction in both inflammatory and neuropathic pain, and has been shown to be beneficial for decreasing pain associated with rheumatoid arthritis, dysmenorrhea (pain during menstruation), inflammatory bowl disease, and neuropathy (Tokuyama 2011). Conversely, excessive levels of omega-6 PUFAs, such as arachidonic acid, are associated with inflammatory activities, an effect that can be offset by the simultaneous consumption of omega-3 PUFAs (Surette 2008).
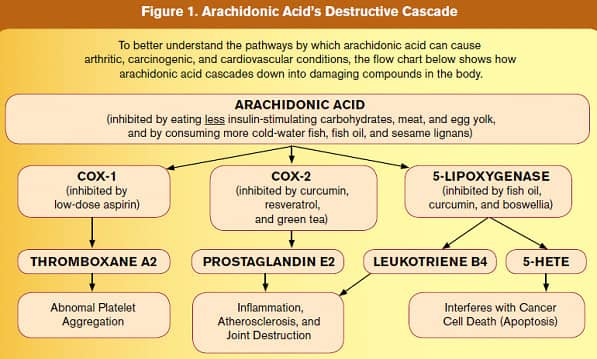 |
| Figure 1: Arachidonic Acid’s Destructive Cascade |
In response to arachidonic acid overload, the body increases its production of enzymes like 5-lipoxygenase (5-LOX) to degrade arachidonic acid. Not only do 5-LOX products directly stimulate cancer cell propagation, but the breakdown products that 5-LOX produces from arachidonic acid (such as leukotriene B4, 5-HETE, and hydroxylated fatty acids) cause tissue destruction, chronic inflammation, and increased resistance of tumor cells to apoptosis (programmed cell destruction) (Poff 2004; Bachi 2009; Larré 2008; Sundaram 2006; Zhi 2003; Penglis 2000; Rubinsztajn 2003; Subbarao 2004; Laufer 2003; Julémont 2004).
It is important to understand that 5-LOX is not the only dangerous enzyme the body produces to break down arachidonic acid. As can be seen in Figure 1, both cyclooxygenase-1 and cyclooxygenase-2 (COX-1 and COX-2) also participate in the degradation of arachidonic acid.
COX-1 causes the production of thromboxane A2, which can promote abnormal arterial blood clotting (thrombosis), resulting in heart attack and stroke (Nakahata 2008). COX-2 is directly involved in cancer cell propagation, while its breakdown product (prostaglandin E2) promotes chronic inflammation (Suzuki 2011). Most health-conscious people already inhibit the COX-1 and COX-2 enzymes by taking low-dose aspirin, curcumin, green tea, and various flavonoids such as resveratrol.
A more integrative approach to this problem, however, would be to also reduce levels of arachidonic acid, which is the precursor of 5-HETE and leukotriene.
Experts believe that another mechanism responsible for the anti-inflammatory effect of omega-3 PUFAs has something to do with their metabolites (i.e., resolvins), which possess potent anti-inflammatory properties (Serhan 2005). Resolvins bind and activate receptors on immune cells and neuronal cells leading to alterations in pain transduction in the spinal cord and a dampened inflammatory response (Serhan 2002; Ji 2011). The positive effect of omega-3’s on neuropathic pain has been partially explained by their ability to block voltage-gated sodium channels (VGSCs), ultimately interfering with pain signaling (Ko 2010).
Because omega-3 PUFAs are associated with positive effects on cognition, mood, and behavior (Kidd 2007), they may also be beneficial to central pain processing (Manson 2010). Omega-3 supplementation can also help reduce anti-inflammatory analgesic consumption (Goldberg 2007), which might in turn reduce the associated risk of developing gastrointestinal side effects. Since omega-3’s do not interact with most analgesic drugs, some experts recommend their concomitant use (along with conventional analgesic therapies) for the management of both inflammatory and neuropathic pain (Shapiro 2003).
Gamma Linolenic Acid – the beneficial omega-6 fatty acid
Gamma linolenic acid (GLA) is a plant-derived omega-6 most abundant in seeds of an Eastern flower known as borage. Although a member of the omega-6 family, it is metabolized differently than other omega-6s.
GLA plays an important role in modulating inflammation throughout the body, especially when incorporated into the membranes of immune system cells (Johnson 1997; Ziboh 2004). Early in 2010, a team of Taiwanese researchers discovered that GLA regulates the inflammatory "master molecule" nuclear factor-kappaB or Nf-kB, preventing it from switching on genes for inflammatory cytokines in cell nuclei (Chang 2010).
A separate mechanism by which GLA and other beneficial fatty acids reduce inflammation is by activating the powerful peroxisome proliferator-activated receptor (PPAR) system (Hontecillas 2009). PPARs are intracellular receptors that modulate cell metabolism and responses to inflammation. The class of antidiabetic drugs called thiazolidinediones (such as Actos® or pioglitazone) acts by targeting PPARs—but unlike GLA, they can be deadly.
In studies, GLA has been shown to relieve pain that results from a variety of conditions, including neuropathy, breast pain, and rheumatoid arthritis (Horrobin 1993; Ranieri 2009; Hansen 1983) (Chaggar 2009).
Vitamins
- B Vitamins – Vitamins B1 (thiamine), B6 (pyridoxine), and B12 (cyanocobalamin/ methylcobalamin) are not only beneficial for managing pain that may result from a vitamin B deficiency, but are also effective (alone or in combination) with other conventional medications for various painful diseases (e.g., degenerative spine disease, rheumatic diseases, low-back pain, and tonsillectomy pain) (Proctor 2001; Koike 2006; Ponce-Monter 2012). The administration of a mixture of vitamins B1, B6, and B12 has also been shown to reduce neuropathic pain in humans and animals (Caram-Salas 2006), and can therefore help treat peripheral neuropathies (Medina-Santillan 2004). Benfotiamine (a better absorbed derivative of vitamin B1) has also been suggested for reducing inflammatory and neuropathic pain in humans (Sanchez-Ramirez 2006).Evidence suggests that neuropathic pain plays a considerable role in many cases of chronic pain, and that B-vitamins primarily provide relief by targeting pathways associated with central neural pain processing (Mibielli 2009).
- Vitamin C – Vitamin C (ascorbic acid), a versatile antioxidant, may act as another natural shield against pain. Accumulating evidence indicates that free radicals play a role in the exaggeration of pain hypersensitivity (Lu 2011). Vitamin C has been linked to a rapid and consistent anti-nociceptive (pain–relieving) effect in animal studies (Rosa 2005). A 2011 animal study revealed that the administration of the antioxidants Vitamin C and E inhibited pain related to peripheral injury. The authors concluded, "supplementation or treatment with both vitamins might be an option in patients suffering from specific pain states" (Lu 2011). Administration of vitamin C also reduces spontaneous pain associated with postherpetic neuralgia, which is a type of peripheral neuropathic pain (Chen 2009). Prophylactic vitamin C supplementation has also been linked to a 5-fold decrease in the incidence of complex regional pain syndrome among patients who recently underwent foot/ankle surgery (compared to no treatment) (Besse 2009).
- Vitamin D – Vitamin D is a prohormone version of an important hormone called 1,25-dihydroxycholecalciferol or 1,25-dihydroxy vitamin D, also known as calcitriol (Dusso 2005). Vitamin D, once converted into calcitriol, inhibits inflammation by regulating some of the genes responsible for producing pro-inflammatory mediators (i.e., cytokines) (Manson 2010). In addition to being associated with pain due to bone softening (i.e., osteomalacia), vitamin D deficiency has also been linked to fibromyalgia, chronic widespread pain (CWP), and an unusual pain syndrome characterized by musculoskeletal and bone pain (Gloth 2004; Manson 2010). In addition, administration of vitamin D was found to significantly reduce pain for women with chronically painful periods in a randomized double-blind placebo controlled study (Lasco 2012). Life Extension recommends routine vitamin D deficiency testing for all individuals with pain complaints. If vitamin D levels are low, vitamin D supplementation may result in significant improvements in pain (Selfridge 2010). Life Extension suggests that blood levels of 25-hydroxyvitamin D should be kept between 50 and 80 ng/mL for optimal health.
- Vitamin E – Vitamin E has been associated with a reduction in the severity of cyclic breast pain, a condition affecting as much as 69% of women (Pruthi 2010). It is also effective at relieving the pain associated with menstrual cramps (Ziaei 2005). In experimental models, supplementation with tocotrienols (a certain type of vitamin E) has been shown to improve neuropathic pain intensity associated with both diabetic and alcoholic neuropathy in animal models (Kuhad 2009; Tiwari 2009). The analgesic effects of vitamin E may be partially explained through its antioxidant properties, which involve blocking the production of reactive oxygen species (ROS) that are involved in neuropathic pain. Vitamin E’s analgesic effect may also be related to its ability to make the brain less sensitive to pain (Kim 2006).
Miscellaneous Natural Compounds
- Curcumin ‒ Curcumin is a major component of turmeric, a spice that gives Indian curry its distinct color and taste. In addition to its culinary use, curcumin has long been part of traditional medicine and appreciated for its anti-inflammatory properties (Razavi 2021). Specifically, curcumin has been shown to reduce levels of the inflammatory mediators TNF-α, IL-1β, and IL-6, which contribute to nociceptor hypersensitivity (Singh 2018). Since curcumin has been shown to have analgesic effects in numerous clinical trials, it may be useful for a variety of pain conditions. For example, systematic reviews of clinical trials have shown curcumin use may improve pain in osteoarthritis and rheumatoid arthritis (Bagherniya 2021; Shokri-Mashhadi 2021). Curcumin is also used in India for managing traumatic and postoperative pain and has been shown to reduce chronic neuropathic pain in animal models (Du 2021; Saffarpour 2021; Abdelrahman 2021). One potential challenge with curcumin use is its limited oral bioavailability (Mahmood 2015). Upon ingestion, curcumin is rapidly metabolized into various related molecules, which may not provide the same benefits as free curcumin (Kurita 2013). Researchers have explored different ways to improve the bioavailability of curcumin, including combining with galactomannans (fiber) from fenugreek to form curcumagalactomannosides. In one double-blinded crossover study with 50 participants, the novel curcumin preparation had 45.5-fold higher bioavailability of free curcuminoids than unformulated curcumin (Kumar 2016).
- Boswellia serrata ‒ Boswellia serrata is a plant native to India that has been used for centuries in Ayurvedic medicine. The plant’s resin contains numerous terpenes and four major pentacyclic triterpenic acids knowns as bowellic acids (eg, acetyl-11-keto-β-boswellic acid, or AKBA). These boswellic acids have anti-inflammatory activity, including inhibition of 5-LOX, IL-1β, and TNF-α (Siddiqui 2011). Boswellia extracts have been shown in systematic reviews of clinical trials to improve pain in osteoarthritis (Yu 2020; Cameron 2014). A small placebo-controlled crossover study demonstrated that a single dose of Boswellia serrata (250 mg) increased pain tolerance in healthy adults (Prabhavathi 2014). In a report of four patients with chronic cluster headaches, Boswellia extract was associated with reduced frequency and intensity of headaches (Lampl 2012).
- Black Sesame ‒ Sesame is a flowering plant that is grown in tropical regions worldwide. Its seeds and oils are often used in food and may also possess antinociceptive and anti-inflammatory activity (Monteiro 2014). Sesame oil was shown to reverse the overexpression of IL-1β and TNF-α in an animal model of neuroinflammation (Mohamed 2021). In a trial of 50 patients with osteoarthritis of the knee, sesame supplementation significantly reduced pain intensity compared with placebo (Eftekhar Sabat 2013). And in study with 88 subjects with acute musculoskeletal pain, treatment with a proprietary mixture of curcumin, Boswellia, and black sesame oil extracts resulted in pain relief comparable to acetaminophen. Interestingly, while both groups experienced similar reduction in sensory pain, the herbal preparation was greater than eight times more effective than acetaminophen at relieving the emotional aspects of dealing with acute pain (Rudrappa 2020).
- Ginger - Ginger (Zingiber officinale) has analgesic and anti-inflammatory properties (Black 2010). Certain wild ginger species have anti-nociceptive characteristics and have been used traditionally to treat toothaches, muscle sprains, and swollen cuts/sores (Khalid 2011). Ginger has effectively relieved pain related to arthritis and exercise-related muscle injury in some research (Black 2010). For menstrual pain relief, ginger has been found to be as effective as conventional analgesics such as ibuprofen (Ozgoli 2009). A 2020 review of the literature concluded that ginger is a “safe and promising” nutrient for reducing pain, although more studies are needed to determine the optimal dosage for long-term use (Rondanelli 2020).
- Five-leaf chaste tree (Vitex negundo L.) and ginger extracts – A proprietary blend of five-leaf chaste tree (Vitex negundo L.) and ginger extracts has demonstrated potent pain-relieving effects. In one clinical trial, 72 adults aged 16 to 60 years with lower back pain were randomized to receive either 200 mg of the blend or placebo twice daily for 30 days. By day 7, participants taking the blend experienced a significant decrease in lower back pain compared with those taking placebo. By day 30, 79% of participants taking the blend experienced a clinically meaningful change in their lower back pain compared to 36% in the placebo group. Participants taking the blend also experienced clinically meaningful improvements in their functional activity and bending flexibility (Srivastava 2024). The same blend also reduced exercised-induced knee discomfort four hours after administration compared with placebo in 40 adults (Srivastava 2023). Vitex negundo L. appears to exert its pain-relieving effects via inhibition of COX and LOX enzymes, thereby decreasing prostaglandin production (Chattopadhyay 2012; Gill 2018).
- Proanthocyanidins – Proanthocyanidins (tannins) belong to a group of chemical compounds called "flavonoids", which provide a variety of beneficial functions for humans (e.g., their well-known antioxidant and anti-inflammatory affect). Grape seed is an especially rich source of proanthocyanidins, which have been associated with symptom reduction in a variety of painful diseases (e.g., diabetic neuropathy and chronic pancreatitis) (Banerjee 2001, de la Iglesia 2010). Other sources of proanthocyanidins include berries, seeds, flowers, and leaves (de la Iglesia 2010). The mechanism(s) by which proanthocyanidins alleviate pain are not well understood, but some evidence indicates that central interaction with dopamine receptors may be involved (DalBo 2006).
- Melatonin – Melatonin is a naturally occurring hormone that is synthesized by the pineal gland and regulated by the environmental light/dark cycle (Kaur 2011). Melatonin can reduce pain through its beneficial effect on sleep, as well as its analgesic properties. It is also a potent antioxidant, and has been shown to reduce the pain associated with a variety of chronically painful conditions (e.g., fibromyalgia, irritable bowel syndrome, and migraine) (Wilhelmsen 2011). A study in infants found that melatonin powerfully relieves pain by suppressing levels of the IL-6 and other inflammatory cytokines (Gitto 2012). Melatonin is such a remarkable compound that its chemical structure may be the basis of new analgesic drugs for the treatment of pain associated with cancer, headache, or even surgical procedures (Srinivasan 2010).
- Methylsulfonylmethane - Methylsulfonylmethane (MSM) is an organic sulfur-containing compound (Debbi 2011) found in a variety of fruits, vegetables, grains, and meats. Among its many beneficial functions, MSM has been shown to display anti-inflammatory and antioxidant properties (AMR 2003). MSM has been successfully used to treat pain associated with osteoarthritis (OA) of the knee (Debbi 2011) and is not typically associated with any significant adverse side effects (Kim LS 2006). When combined with Boswellia seratta MSM significantly reduced the need for NSAIDs compared to placebo among subjects with knee osteoarthritis, suggesting the combination exerted considerable anti-inflammatory action (Notarnicola 2011).
- Korean angelica - Decursinol is a medicinal compound found in the roots of the Korean flower called Angelica gigas Nakai (Korean angelica) (Song 2011). It has been widely utilized in traditional oriental medicine as a treatment regimen for pain associated with menstruation, arthritis, migraine, abdominal pain, and other miscellaneous injuries (Kim 2009). Researchers suggest that decursinol may act in the central nervous system to exert its analgesic effect, or interfere with nociception (Choi 2003). Scientists report laboratory evidence showing that an active constituent derived from Korean Angelica inhibits activation of nuclear factor-kappa B (Nf-kB), a DNA transcription factor that is involved in many inflammatory and disease states (Kim 2006). More recent studies indicated that co-administration of decursinol and acetaminophen resulted in synergistic effects, which enabled acetaminophen to be therapeutic at lower-than-normal doses. This acetaminophen-sparing effect implies that decursinol may inhibit the COX (cyclooxygenase) enzymes (Seo 2009).
- Capsaicin - Capsaicin, the compound that gives chili peppers their spicy taste, also has medicinal value as an over-the-counter topical pain reliever. It is well tolerated, and comes in a variety of formulations such as creams, gels, lotions, patches, and sticks (Robb-Nicholson 2011). It has been shown to be an effective analgesic for low-back pain, as well as chronic pain originating in the muscles, tendons, and ligaments (Chrubasik 2010). Topical capsaicin has also been associated with a significant reduction in neuropathic pain (England 2011). Researchers believe its analgesic effect occurs as a result of its ability to reduce the amount of nerve fibers in the application area (upon long-term administration), as well as its capacity for interfering with nociception (i.e., defunctionalization). Both of these actions ultimately contribute to a local decrease in responsiveness to a wide range of sensory stimuli (Anand 2011; Jones 2011).
- DL-Phenylalanine – While L-phenylalanine is a naturally occurring amino acid that is a precursor to dopamine and related neurotransmitters (Fernstrom 2007), D-phenylalanine appears to slow metabolic breakdown of endogenous opioids (Kitade 1990). DL-phenylalanine, which is a mixture of both stereoisomers, may therefore provide an analgesic and mood-boosting effect. Some limited studies suggest that supplementation with phenylalanine might provide pain relief (Kitade 1990; Donzelle 1981), but larger, well-designed studies have failed to corroborate these early observations (Mitchell 1987; Walsh 1986). Evidence is currently insufficient to draw firm conclusions as to the pain-relieving efficacy of DL-phenylalanine.
Boosting Serotonin Signaling
Saffron & L-Tryptophan – Antidepressant medications provide analgesia via various mechanisms, including by boosting levels of serotonin, which helps the brain control pain sensations (Dharmshaktu 2012). Therefore, since the amino L-tryptophan and bioactive compounds in saffron may modulate serotonergic activity within the brain, some innovative scientists have proposed them as potential central pain relievers (Amin 2012; Ceccherelli 1991).
Hepato-protective Nutrients
N-acetyl-cysteine & milk thistle extract – For those taking high-doses of acetaminophen for pain relief, supplementation with hepato-protective nutrients such as N-acetyl-cysteine and milk thistle extract may provide a means of reducing drug-induced liver damage (Abenavoli 2010; Bajt 2004).
2024
- Apr: Added section on Chinese chaste tree (Vitex negundo L.) and ginger extracts & updated section on ginger in Nutrients
2021
- Oct: Updated section on curcumin in Nutrients
- Oct: Added section on Boswellia serrata to Nutrients
- Oct: Added section on black sesame to Nutrients
2012
- May: Comprehensive update & review
Disclaimer and Safety Information
This information (and any accompanying material) is not intended to replace the attention or advice of a physician or other qualified health care professional. Anyone who wishes to embark on any dietary, drug, exercise, or other lifestyle change intended to prevent or treat a specific disease or condition should first consult with and seek clearance from a physician or other qualified health care professional. Pregnant women in particular should seek the advice of a physician before using any protocol listed on this website. The protocols described on this website are for adults only, unless otherwise specified. Product labels may contain important safety information and the most recent product information provided by the product manufacturers should be carefully reviewed prior to use to verify the dose, administration, and contraindications. National, state, and local laws may vary regarding the use and application of many of the therapies discussed. The reader assumes the risk of any injuries. The authors and publishers, their affiliates and assigns are not liable for any injury and/or damage to persons arising from this protocol and expressly disclaim responsibility for any adverse effects resulting from the use of the information contained herein.
The protocols raise many issues that are subject to change as new data emerge. None of our suggested protocol regimens can guarantee health benefits. Life Extension has not performed independent verification of the data contained in the referenced materials, and expressly disclaims responsibility for any error in the literature.
Abenavoli L, Capasso R, Milic N, et al. Milk thistle in liver diseases: past, present, future. Phytother Res. 2010 Oct;24(10):1423-32.
Abdelrahman KM, Hackshaw KV. Nutritional Supplements for the Treatment of Neuropathic Pain. Biomedicines. Jun 13 2021;9(6) doi:10.3390/biomedicines9060674
Aloisi A, Ceccarelli I, Carlucci M, et al. Hormone replacement therapy in morphine-induced hypogonadic male chronic pain patients. Reproductive Biology and Endocrinology. 2011;9(1):26.
Aloisi AM, Aurilio C, Bachiocco V, et al. Endocrine consequences of opioid therapy. Psychoneuroendocrinology. 2009;34(1).
Amin B and Hosseinzadeh H. Evaluation of aqueous and ethanolic extracts of saffron, Crocus sativus L., and its constituents, safranal and crocin in allodynia and hyperalgesia induced by chronic constriction injury model of neuropathic pain in rats. Fitoterapia. 2012 Mar 28. [Epub ahead of print]
AMR (Alternative Medicine Review). Methylsulfonylmethane (MSM). Monograph. Altern Med Rev. 2003;8(4):438-41.
Anand P, Bley K. Topical capsaicin for pain management: therapeutic potential and mechanisms of action of the new high-concentration capsaicin 8% patch. Br J Anaesth. 2011;107(4):490-502.aspx. Last updated 9/12/2008. Accessed 7/11/2013.
Bachi AL, Kim FJ, Nonogaki S, et al. Leukotriene B4 creates a favorable microenvironment for murine melanoma growth. Mol Cancer Res. 2009 Sep;7(9):1417-24.
Bagherniya M, Darand M, Askari G, Guest PC, Sathyapalan T, Sahebkar A. The Clinical Use of Curcumin for the Treatment of Rheumatoid Arthritis: A Systematic Review of Clinical Trials. Advances in experimental medicine and biology. 2021;1291:251-263. doi:10.1007/978-3-030-56153-6_15
Bajt ML, Knight TR, Lemasters JJ et al. Acetaminophen-induced oxidant stress and cell injury in cultured mouse hepatocytes: protection by N-acetyl cysteine. Toxicol Sci. 2004 Aug;80(2):343-9. Epub 2004 Apr 28.
Bajwa Z, Smith HS. Overview of the treatment of chronic pain. In: UpToDate, Aronson M. (Ed), Waltham, MA, 2012.
Banerjee B, Bagchi D. Beneficial effects of a novel IH636 grape seed proanthocyanidin extract in the treatment of chronic pancreatitis. Digestion. 2001;63(3):203-206.
Bell RF. Food and pain: Should we be more interested in what our patients eat? Pain. 2007;129(1-2):5-7.
Besse JL, Gadeyne S, Galand-Desme S, Lerat JL, Moyen B. Effect of vitamin C on prevention of complex regional pain syndrome type I in foot and ankle surgery. Foot Ankle Surg. 2009;15(4):179-182.
Black CD, Herring MP, Hurley DJ, O'Connor PJ. Ginger (Zingiber officinale) reduces muscle pain caused by eccentric exercise. J Pain. 2010;11(9):894-903.
Bonakdar R, Leopold D. Chapter 34: Integrative Medicine in Rheumatology: An Evidence-Based Approach. In: Firestein: Kelley's Textbook of Rheumatology, 8th ed. Philadelphia PA: Saunders Elsevier 2009.
Bradley LA, Kersh BC, DeBerry JJ, et al. Lessons from fibromyalgia: abnormal pain sensitivity in knee osteoarthritis. Novartis Found Symp. 2004;260:258-70; discussion 270-9.
Cameron M, Chrubasik S. Oral herbal therapies for treating osteoarthritis. The Cochrane database of systematic reviews. May 22 2014;5(5):Cd002947. doi:10.1002/14651858.CD002947.pub2
Caram-Salas NL, Reyes-Garcia G, Medina-Santillan R, Granados-Soto V. Thiamine and cyanocobalamin relieve neuropathic pain in rats: synergy with dexamethasone. Pharmacology. 2006;77(2):53-62.
Ceccherelli F, Diani MM, Altafini L. erative pain treated by intravenous L-tryptophan: a double-blind study versus placebo in cholecystectomized patients. Pain. 1991 Nov;47(2):163-72.
Chaggar PS, Shaw SM, Williams SG. Review article: Thiazolidinediones and heart failure. Diab Vasc Dis Res. 2009 Jul;6(3):146-52.
Chang CS, Sun HL, Lii CK, Chen HW, Chen PY, Liu KL. Gamma-linolenic acid inhibits inflammatory responses by regulating NF-kappaB and AP-1 activation in lipopolysaccharide-induced RAW 264.7 macrophages. Inflammation. 2010 Feb;33(1):46-57.
Chattopadhyay P, Hazarika S, Dhiman S, et al. Vitex negundo inhibits cyclooxygenase-2 inflammatory cytokine-mediated inflammation on carrageenan-induced rat hind paw edema. Pharmacognosy Res. Jul 2012;4(3):134-7. doi:10.4103/0974-8490.99072. https://pubmed.ncbi.nlm.nih.gov/22923950/
Chen JY, Chang CY, Feng PH, Chu CC, So EC, Hu ML. Plasma vitamin C is lower in postherpetic neuralgia patients and administration of vitamin C reduces spontaneous pain but not brush-evoked pain. Clin J Pain. 2009;25(7):562-569.
Choi SS, Han KJ, Lee JK, et al. Antinociceptive mechanisms of orally administered decursinol in the mouse. Life Sci. 2003;73(4):471-485.
Chou R, Fanciullo GJ, Fine PG, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain. 2009;10(2):113-130.
Chrubasik S, Weiser T, Beime B. Effectiveness and safety of topical capsaicin cream in the treatment of chronic soft tissue pain. Phytother Res. 2010;24(12):1877-1885.
Cleveland Clinic. Acute vs. Chronic Pain. Treatments & Procedures page. Available at:
Cohen S., Raja S., Chapter 29 – Pain. In: Goldman: Goldman's Cecil Medicine, 24th ed. Pg 133. Copyright © 2011 Saunders, An Imprint of Elsevier. Philadelphia, PA.
Coluzzi F, Berti M. Change Pain: changing the approach to chronic pain. Minerva Med. 2011;102(4):289-307.
Costigan M, Scholz J, Woolf CJ. Neuropathic pain: a maladaptive response of the nervous system to damage. Annu Rev Neurosci. 2009;32:1-32.
DalBo S, Jurgensen S, Horst H, et al. Analysis of the antinociceptive effect of the proanthocyanidin-rich fraction obtained from Croton celtidifolius barks: evidence for a role of the dopaminergic system. Pharmacol Biochem Behav. 2006 Oct;85(2):317-23. Epub 2006 Oct 9.
de la Iglesia R, Milagro FI, Campion J, Boque N, Martinez JA. Healthy properties of proanthocyanidins. Biofactors. 2010;36(3):159-168.
Debbi EM, Agar G, Fichman G, et al. Efficacy of methylsulfonylmethane supplementation on osteoarthritis of the knee: a randomized controlled study. BMC Complement Altern Med. 2011;11:50.
Dharmshaktu P, Tayal V, and Kalra BS. Efficacy of antidepressants as analgesics: a review. J Clin Pharmacol. 2012 Jan;52(1):6-17. Epub 2011 Mar 17.
Donzelle G, Bernard L, Deumier R, et al. [Curing trial of complicated oncologic pain by D-phenylalanine (author's transl)]. Anesth Analg (Paris). 1981;38(11-12):655-8.
Du J, Deng Y, Qiu Z, et al. Curcumin Alleviates Chronic Pain and Improves Cognitive Impairment via Enhancing Hippocampal Neurogenesis in Sciatic Nerve Constriction Rats. J Pain Res. 2021;14:1061-1070. doi:10.2147/jpr.S299604
Dusso AS, Brown AJ, Slatopolsky E. Vitamin D. American Journal of Physiology - Renal Physiology. July 1, 2005 2005;289(1):F8-F28.
Edlund MJ, Steffick D, Hudson T, Harris KM, Sullivan M. Risk factors for clinically recognized opioid abuse and dependence among veterans using opioids for chronic non-cancer pain. Pain. 2007;129(3):355-362.
Eftekhar Sadat B, Khadem Haghighian M, Alipoor B, Malek Mahdavi A, Asghari Jafarabadi M, Moghaddam A. Effects of sesame seed supplementation on clinical signs and symptoms in patients with knee osteoarthritis. Int J Rheum Dis. Oct 2013;16(5):578-82. doi:10.1111/1756-185x.12133
Ejaz P, Bhojani K, Joshi VR. NSAIDs and kidney. J Assoc Physicians India. 2004 Aug;52:632-40.
England J, Wagner T, Kern KU, Roth-Daniek A, Sell A. The capsaicin 8% patch for peripheral neuropathic pain. Br J Nurs. 2011;20(15):926-931.
Fernstrom JD and Fernstrom MH. Tyrosine, phenylalanine, and catecholamine synthesis and function in the brain. J Nutr. 2007 Jun;137(6 Suppl 1):1539S-1547S; discussion 1548S.
Food and Drug Administration (FDA). Acetaminophen: background and overview. Meeting material from the June 29, 2009, joint meeting of the Drug Safety and Risk Management Advisory Committee with the Anesthetic and Life Support Advisory Committee and Nonprescription Drug Advisory Committee. Silver Spring, MD, 2009.
Friedrich MJ. Research yields new insights into mechanisms and treatment of pain: JAMA. 2012 Jan 18;307(3):239-41.
Gill BS, Mehra R, Navgeet, Kumar S. Vitex negundo and its medicinal value. Molecular biology reports. Dec 2018;45(6):2925-2934. doi:10.1007/s11033-018-4421-3. https://pubmed.ncbi.nlm.nih.gov/30311123/
Gitto E, Aversa S, Salpietro CD, et al. Pain in neonatal intensive care: role of melatonin as an analgesic antioxidant. J Pineal Res. 2012 Apr;52(3):291-5.
Gloth FM, 3rd, Greenough WB, 3rd. Vitamin D deficiency as a contributor to multiple forms of chronic pain: Mayo Clin Proc. 2004 May;79(5):696, 699; author reply 699.
Goldberg RJ, Katz J. A meta-analysis of the analgesic effects of omega-3 polyunsaturated fatty acid supplementation for inflammatory joint pain. Pain. 2007;129(1-2):210-223.
Hansen TM, Lerche A, Kassis V, et al. Treatment of rheumatoid arthritis with prostaglandin E1 precursors cis-linoleic acid and gamma-linolenic acid. Scand J Rheumatol. 1983;12(2):85-8.
Hassett AL, Williams DA. Non-pharmacological treatment of chronic widespread musculoskeletal pain. Best Pract Res Clin Rheumatol. 2011;25(2):299-309.
Hersh EV, Pinto A, Moore PA. Adverse drug interactions involving common prescription and over-the-counter analgesic agents. Clin Ther. 2007;29(97):2477-97.
Hontecillas R, O’Shea M, Einerhand A, Diguardo M, Bassaganya-Riera J. Activation of PPAR gamma and alpha by punicic acid ameliorates glucose tolerance and suppresses obesity-related inflammation. J Am Coll Nutr. 2009 Apr;28(2):184-95.
Horrobin DF. The effects of gamma-linolenic acid on breast pain and diabetic neuropathy: possible non-eicosanoid mechanisms. Prostaglandins Leukot Essent Fatty Acids. 1993 Jan;48(1):101-4. http://my.clevelandclinic.org/services/pain_management/hic_acute_vs_chronic_pain.
Ji RR, Xu ZZ, Strichartz G, Serhan CN. Emerging roles of resolvins in the resolution of inflammation and pain. Trends Neurosci. 2011;34(11):599-609.
Johnson MM, Swan DD, Surette ME, et al. Dietary supplementation with gamma-linolenic acid alters fatty acid content and eicosanoid production in healthy humans. J Nutr. 1997 Aug;127(8):1435-44.
Jones VM, Moore KA, Peterson DM. Capsaicin 8% topical patch (Qutenza)--a review of the evidence. J Pain Palliat Care Pharmacother. 2011;25(1):32-41.
Julémont F, Dogné, Pirotte B, et al. Recent development in the field of dual COX/5-LOS inhibitors. Mini Rev Med Chem. 2004;4(6):633-8.
Katz N, Mazer NA. The impact of opioids on the endocrine system. Clin J Pain. 2009;25(2):170-175.
Kaur C. The pineal hormone melatonin in health and disease. Recent Pat Endocr Metab Immune Drug Discov. 2011;5(2):78-9.
Khalid MH, Akhtar MN, Mohamad AS, et al. Antinociceptive effect of the essential oil of Zingiber zerumbet in mice: possible mechanisms. J Ethnopharmacol. 2011;137(1):345-351.
Kidd PM. Omega-3 DHA and EPA for cognition, behavior, and mood: clinical findings and structural-functional synergies with cell membrane phospholipids. Altern Med Rev. 2007;12(3):207-227.
Kim HK, Kim JH, Gao X, et al. Analgesic effect of vitamin E is mediated by reducing central sensitization in neuropathic pain. Pain. 2006a;122(1-2):53-62.
Kim JH, Jeong JH, Jeon ST, et al. Decursin inhibits induction of inflammatory mediators by blocking nuclear factor-kappaB activation in macrophages. Mol Pharmacol. 2006b Jun;69(6):1783-90. Epub 2006 Mar 1.
Kim KM, Kim MJ, Kang JS. Absorption, distribution, metabolism, and excretion of decursin and decursinol angelate from Angelica gigas Nakai. J Microbiol Biotechnol. 2009;19(12):1569-1572.
Kim LS, Axelrod LJ, Howard P, Buratovich N, Waters RF. Efficacy of methylsulfonylmethane (MSM) in osteoarthritis pain of the knee: a pilot clinical trial. Osteoarthritis Cartilage. 2006;14(3):286-94.
Kitade T, Odahara Y, Shinohara S, et al. Studies on the enhanced effect of acupuncture analgesia and acupuncture anesthesia by D-phenylalanine (2nd report)--schedule of administration and clinical effects in low back pain and tooth extraction. Acupunct Electrother Res. 1990;15(2):121-35.
Ko GD, Nowacki NB, Arseneau L, Eitel M, Hum A. Omega-3 fatty acids for neuropathic pain: case series. Clin J Pain. 2010;26(2):168-172.
Koike H, Watanabe H, Inukai A, et al. Myopathy in thiamine deficiency: analysis of a case. J Neurol Sci. 2006;249(2):175-179.
Kuhad A, Chopra K. Tocotrienol attenuates oxidative-nitrosative stress and inflammatory cascade in experimental model of diabetic neuropathy. Neuropharmacology. 2009;57(4):456-462.
Kumar D, Jacob D, Ps S, et al. Enhanced bioavailability and relative distribution of free (unconjugated) curcuminoids following the oral administration of a food-grade formulation with fenugreek dietary fibre: A randomised double-blind crossover study. Journal of Functional Foods. 2016/04/01/ 2016;22:578-587. doi:https://doi.org/10.1016/j.jff.2016.01.039
Kurita T, Makino Y. Novel curcumin oral delivery systems. Anticancer research. Jul 2013;33(7):2807-21.
Lampl C, Haider B, Schweiger C. Long-term efficacy of Boswellia serrata in four patients with chronic cluster headache. Cephalalgia. Jul 2012;32(9):719-22. doi:10.1177/0333102412451357
Larré S, Tran N, Fan C, et al. PGE2 and LTB4 tissue levels in benign and cancerous prostates. Prostaglandins Other Lipid Mediat. 2008 Dec;87(1-4):14-9.
Lasco A, Catalano A, Benvenga S. Improvement of primary dysmenorrhea caused by a single oral dose of vitamin D: results of a randomized, double-blind, placebo-controlled study. Arch Intern Med. 2012 Feb 27;172(4):366-7.
Laufer S. Role of eicosanoids in structural degradation in osteoarthritis. Curr Opin Rheumatol. 2003 Sep;15(5):623-7.
Lu R, Kallenborn-Gerhardt W, Geisslinger G, Schmidtko A. Additive antinociceptive effects of a combination of vitamin C and vitamin E after peripheral nerve injury. PLoS One. 2011;6(12):e29240. Epub 2011 Dec 14.
Lumley MA, Cohen JL, Borszcz GS, et al. Pain and emotion: a biopsychosocial review of recent research. J Clin Psychol. 2011;67(9):942-968.
Mahmood K, Zia KM, Zuber M, Salman M, Anjum MN. Recent developments in curcumin and curcumin based polymeric materials for biomedical applications: A review. International journal of biological macromolecules. Nov 2015;81:877-90. doi:10.1016/j.ijbiomac.2015.09.026
Manson JE. Pain: sex differences and implications for treatment. Metabolism. 2010;59(1):S16-20.
McCleane G. Antidepressants as Analgesics. CNS Drugs, Volume 22, Number 2, 2008 , pp. 139-156(18)
Mease PJ, Hanna S, Frakes EP, et al. Pain mechanisms in osteoarthritis: understanding the role of central pain and current approaches to its treatment. J Rheumatol. 2011 Aug;38(8):1546-51.
MedicineNet.com Chronic Pain. Available at: http://www.medicinenet.com/chronic_pain/article.htm Accessed 4/19/2012.
MedicineNet.com Chronic Pain. Available at: http://www.medicinenet.com/chronic_pain/article.htm Accessed 5/2/2012.
Medina-Santillan R, Morales-Franco G, Espinoza-Raya J, Granados-Soto V, Reyes-Garcia G. Treatment of diabetic neuropathic pain with gabapentin alone or combined with vitamin B complex. preliminary results. Proc West Pharmacol Soc. 2004;47:109-112.
MedlinePlus. Pain. Available at: http://www.nlm.nih.gov/medlineplus/pain.html. Updated 4/27/2012. Accessed 5/2/2012.
Merza Z. Chronic use of opioids and the endocrine system. Horm Metab Res. 2010;42(9):621-626.
Mibielli MA, Geller M, Cohen JC, et al. Diclofenac plus B vitamins versus diclofenac monotherapy in lumbago: the DOLOR study. Curr Med Res Opin. 2009 Nov;25(11):2589-99.
Mitchell MJ, Daines GE, and Thomas BL. Effect of L-tryptophan and phenylalanine on burning pain threshold. Phys Ther. 1987 Feb;67(2):203-5.
Mohamed EA, Ahmed HI, Zaky HS, Badr AM. Sesame oil mitigates memory impairment, oxidative stress, and neurodegeneration in a rat model of Alzheimer's disease. A pivotal role of NF-κB/p38MAPK/BDNF/PPAR-γ pathways. Journal of ethnopharmacology. Mar 1 2021;267:113468. doi:10.1016/j.jep.2020.113468
Monteiro EM, Chibli LA, Yamamoto CH, et al. Antinociceptive and anti-inflammatory activities of the sesame oil and sesamin. Nutrients. May 12 2014;6(5):1931-44. doi:10.3390/nu6051931
Nakahata N et al. Thromboxane A2: physiology/pathophysiology, cellular signal transduction and pharmacology. Pharmacol Ther. 2008 Apr;118(1):18-35.
National Institute of Health (NIH). Aspirin: AHFS Consumer Medication Information. PubMed Health [Internet]. Bethesda (MD): National Library of Medicine (US); [Last updated March 2011; Accessed April 2012]
NINDS (National Institute of Neurological Disorders and Stroke. Pain: Hope Through Research. Available at: http://www.ninds.nih.gov/disorders/chronic_pain/detail_chronic_pain.htm Accessed 5/4/2012.
Notarnicola A, Tafuri S, Fusaro L, et al. The "MESACA" study: methylsulfonylmethane and boswellic acids in the treatment of gonarthrosis. Adv Ther. 2011 Oct;28(10):894-906. Epub 2011 Oct 7.
Okie S. A flood of opioids, a rising tide of deaths. N Engl J Med. 2010;363(21):1981-1985.
Ozgoli G, Goli M, Moattar F. Comparison of effects of ginger, mefenamic acid, and ibuprofen on pain in women with primary dysmenorrhea. J Altern Complement Med. 2009;15(2):129-132.
Penglis PS, Cleland LG, Demasi M, Caughey GE, James MJ. Differential regulation of prostaglandin E2 and thromboxane A2 production in human monocytes: implications for the use of cyclooxygenase inhibitors. J Immunol. 2000 Aug 1;165(3):1605-11.
Peterson K, McDonagh M, Thakurta S, et al. Drug Class Review: Nonsteroidal Antiinflammatory Drugs (NSAIDs): Final Update 4 Report. National Institute of Health (NIH) PubMed Health. Bethesda (MD): National Library of Medicine (US).
Poff CD, Balazy M. Drugs that target lipoxygenases and leukotrienes as emerging therapies for asthma and cancer. Curr Drug Targets Inflamm Allergy. 2004 Mar;3(1):19-33.
Ponce-Monter HA, Ortiz MI, Garza-Hernandez AF, et al. Effect of diclofenac with B vitamins on the treatment of acute pain originated by lower-limb fracture and surgery. Pain Res Treat. 2012;104782:31.
Prabhavathi K, Chandra US, Soanker R, Rani PU. A randomized, double blind, placebo controlled, cross over study to evaluate the analgesic activity of Boswellia serrata in healthy volunteers using mechanical pain model. Indian J Pharmacol. Sep-Oct 2014;46(5):475-9. doi:10.4103/0253-7613.140570
Proctor ML, Murphy PA. Herbal and dietary therapies for primary and secondary dysmenorrhoea. Cochrane Database Syst Rev. 2001;3.
Pruthi S, Wahner-Roedler DL, Torkelson CJ, et al. Vitamin E and evening primrose oil for management of cyclical mastalgia: a randomized pilot study. Altern Med Rev. 2010;15(1):59-67.
Ranieri M, Sciuscio M, Cortese AM, et al. The use of alpha-lipoic acid (ALA), gamma linolenic acid (GLA) and rehabilitation in the treatment of back pain: effect on health-related quality of life. Int J Immunopathol Pharmacol. 2009 Jul-Sep;22(3 Suppl):45-50.
Razavi BM, Ghasemzadeh Rahbardar M, Hosseinzadeh H. A review of therapeutic potentials of turmeric (Curcuma longa) and its active constituent, curcumin, on inflammatory disorders, pain, and their related patents. Phytotherapy research : PTR. Jul 26 2021;doi:10.1002/ptr.7224
Robb-Nicholson C. Ask the doctor. I have pain from osteoarthritis in both knees. I'm curious about the cream made from a substance in hot peppers. How does it relieve pain? Harv Womens Health Watch. 2011;19(2):8.
Rondanelli M, Fossari F, Vecchio V, et al. Clinical trials on pain lowering effect of ginger: A narrative review. Phytother Res. Nov 2020;34(11):2843-2856. doi:10.1002/ptr.6730. https://pubmed.ncbi.nlm.nih.gov/32436242/
Rosa KA, Gadotti VM, Rosa AO, Rodrigues AL, Calixto JB, Santos AR. Evidence for the involvement of glutamatergic system in the antinociceptive effect of ascorbic acid. Neurosci Lett. 2005;381(1-2):185-188.
Rubinsztajn R, Wronska J, Chazan R. Urinary leukotriene E4 concentration in patients with bronchial asthma and intolerance of non-steroids anti-inflammatory drugs before and after oral aspirin challenge. Pol Arch Med Wewn. 2003 Aug;110(2):849-54.
Rudrappa GH, Chakravarthi PT, Benny IR. Efficacy of high-dissolution turmeric-sesame formulation for pain relief in adult subjects with acute musculoskeletal pain compared to acetaminophen: A randomized controlled study. Medicine. Jul 10 2020;99(28):e20373. doi:10.1097/md.0000000000020373
Ruskin DN, Kawamura M, Masino SA. Reduced pain and inflammation in juvenile and adult rats fed a ketogenic diet. PLoS One. 2009;4(12).
Saccomano S, Deluca DA. Too toxic. Nurs Manage. 2008;39(9):32A-H.
Saffarpour S, Janzadeh A, Rahimi B, Ramezani F, Nasirinezhad F. Chronic nanocurcumin treatment ameliorates pain-related behavior, improves spatial memory, and reduces hippocampal levels of IL-1β and TNFα in the chronic constriction injury model of neuropathic pain. Psychopharmacology (Berl). Mar 2021;238(3):877-886. doi:10.1007/s00213-020-05739-x
Sanchez-Ramirez GM, Caram-Salas NL, Rocha-Gonzalez HI, et al. Benfotiamine relieves inflammatory and neuropathic pain in rats. Eur J Pharmacol. 2006;530(1-2):48-53.
Selfridge NJ. Vitamin D and Pain: Making Sense of It All. Alternative Medicine Alert. 2010;13(7):77-78.
Seo YJ, Kwon MS, Park SH, et al. The analgesic effect of decursinol. Arch Pharm Res. 2009;32(6):937-943.
Serhan C, Hong S, Gronert K, et al. A Family of Bioactive Products of Omega-3 Fatty Acid Transformation Circuits Initiated by Aspirin Treatment that Counter Proinflammation Signals October 21, 2002 // JEM vol. 196 no. 8 1025-1037
Serhan CN. Novel eicosanoid and docosanoid mediators: resolvins, docosatrienes, and neuroprotectins. Curr Opin Clin Nutr Metab Care. 2005;8(2):115-121.
Shapiro H. Could n-3 polyunsaturated fatty acids reduce pathological pain by direct actions on the nervous system? Prostaglandins Leukot Essent Fatty Acids. 2003;68(3):219-224.
Shokri-Mashhadi N, Bagherniya M, Askari G, Sathyapalan T, Sahebkar A. A Systematic Review of the Clinical Use of Curcumin for the Treatment of Osteoarthritis. Advances in experimental medicine and biology. 2021;1291:265-282. doi:10.1007/978-3-030-56153-6_16
Siddiqui MZ. Boswellia serrata, a potential antiinflammatory agent: an overview. Indian journal of pharmaceutical sciences. May 2011;73(3):255-61. doi:10.4103/0250-474X.93507
Singh AK, Kumar S, Vinayak M. Recent development in antihyperalgesic effect of phytochemicals: anti-inflammatory and neuro-modulatory actions. Inflamm Res. Aug 2018;67(8):633-654. doi:10.1007/s00011-018-1156-5
Smith HS. Pain Taxonomy. In: The Neurologic Basis for Pain, Pappagalo M (Ed), McGraw-Hill, New York 2005. p.289.
Song JS, Chae J-W, Lee K-R, et al. Pharmacokinetic characterization of decursinol derived from Angelica gigas Nakai in rats. Xenobiotica. 2011;41(10):895-902.
Srinivasan V, Pandi-Perumal SR, Spence DW, et al. Potential use of melatonergic drugs in analgesia: mechanisms of action. Brain Res Bull. 2010;81(4-5):362-71.
Srivastava S, Girandola RN. Effect of E-PR-01 on Activity-Induced Acute Knee Joint Discomfort in Healthy Individuals: A Randomized, Placebo-Controlled, Double-Blind, Cross-Over Study. J Pain Res. 2023;16:2141-2153. doi:10.2147/jpr.S412018. https://pubmed.ncbi.nlm.nih.gov/37384126/
Srivastava S, Karvir S, Girandola RN. Effect of E-PR-01 on non-specific low back pain in the adult population: A randomized, double-blind, placebo-controlled, parallel-group trial. J Back Musculoskelet Rehabil. 2024;37(2):487-502. doi:10.3233/bmr-230197. https://pubmed.ncbi.nlm.nih.gov/38073372/
Subbarao K, Jala VR, Mathis S, et al. Role of leukotriene B4 receptors in the development of atherosclerosis: potential mechanisms. Arterioscler Thromb Vasc Biol. 2004 Feb;24(2):369-75.
Sundaram S, Ghosh J. Expression of 5-oxoETE receptor in prostate cancer cells: critical role in survival. Biochem BiophysRes Commun. 2006 Jan 6;339(1):93-8.
Surette ME. The science behind dietary omega-3 fatty acids. Cmaj. 2008;178(2):177-180.
Suzuki J, Ogawa M, Watanabe R, et al, Roles of prostaglandin E2 in cardiovascular diseases. Int Heart J. 2011;52(5):266-9.
Tall JM, Raja SN. Dietary constituents as novel therapies for pain. Clin J Pain. 2004;20(1):19-26.
Tennant F. A Diet for Patients With Chronic Pain. Practical Pain Management. 2011;11(6):1-2. Available at: http://www.practicalpainmanagement.com/treatments/complementary/diet-patients-chronic-pain
Tiwari V, Kuhad A, Chopra K. Tocotrienol ameliorates behavioral and biochemical alterations in the rat model of alcoholic neuropathy. Pain. 2009;145(1-2):129-135.
Tokuyama S, Nakamoto K. Unsaturated fatty acids and pain. Biol Pharm Bull. 2011;34(8):1174-1178.
Vo, P, Marx, S, Penles, L. Health-related quality of life (HRQoL) among patients experiencing acute and chronic moderate-to-moderately-severe pain: results from a survey of 606 pain patients in the United States. Paper presented at: American Pain Society Annual Meeting; May 8-10, 2008; Tampa, Florida.
Von Korff M, Kolodny A, Deyo RA, Chou R. Long-term opioid therapy reconsidered. Ann Intern Med. 2011;155(5):325-328.
Vorobeychik Y, Gordin V, Mao J, Chen L. Combination therapy for neuropathic pain: a review of current evidence. CNS Drugs. 2011;25(12):1023-1034.
Vuong C, Van Uum SH, O'Dell LE, Lutfy K, Friedman TC. The effects of opioids and opioid analogs on animal and human endocrine systems. Endocr Rev. 2010;31(1):98-132.
Walsh NE, Ramamurthy S, Schoenfeld L, et al. Analgesic effectiveness of D-phenylalanine in chronic pain patients. Arch Phys Med Rehabil. 1986 Jul;67(7):436-9.
Weir MR. Renal effects of nonselective NSAIDs and coxibs. Cleve Clin J Med. 2002;69 Suppl 1:SI53-8.
Wilcox CM, Cryer B, Triadafilopoulos G. Patterns of use and public perception of over-the-counter pain relievers: focus on nonsteroidal antiinflammatory drugs. J Rheumatol. 2005;32(11):2218-24.
Wilhelmsen M, Amirian I, Reiter RJ, Rosenberg J, Gogenur I. Analgesic effects of melatonin: a review of current evidence from experimental and clinical studies. J Pineal Res. 2011;51(3):270-7.
Woodall WS. Opioids & the endocrine system. Adv NPs PAs. 2011;2(11):25-27.
Woodcock J. A difficult balance--pain management, drug safety, and the FDA. N Engl J Med. 2009;361(22):2105-7.
World Health Organization. Cancer pain releif. World Health Organization; Geneva, 1990.
Yalcin L, Choucair-Jaafar N, Benbouzid M, et al. beta(2)-adrenoceptors are critical for antidepressant treatment of neuropathic pain. Ann Neurol. 2009 Feb;65(2):218-25. Ann Neurol. 2009 Feb;65(2):218-25.
Yu G, Xiang W, Zhang T, Zeng L, Yang K, Li J. Effectiveness of Boswellia and Boswellia extract for osteoarthritis patients: a systematic review and meta-analysis. BMC Complement Med Ther. Jul 17 2020;20(1):225. doi:10.1186/s12906-020-02985-6
Zhi H, Zhang J, Hu G, et al. The deregulation of arachidonic acid metabolism-related genes in human esophageal squamous cell carcinoma. Int J Cancer. 2003 Sep 1;106(3):327-33.
Ziaei S, Zakeri M, Kazemnejad A. A randomised controlled trial of vitamin E in the treatment of primary dysmenorrhoea. Bjog. 2005;112(4):466-469.
Ziboh VA, Naguwa S, Vang K, et al. Suppression of leukotriene B4 generation by ex-vivo neutrophils isolated from asthma patients on dietary supplementation with gammalinolenic acid-containing borage oil: possible implication in asthma. Clin Dev Immunol. 2004 Mar;11(1):13-21.
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun